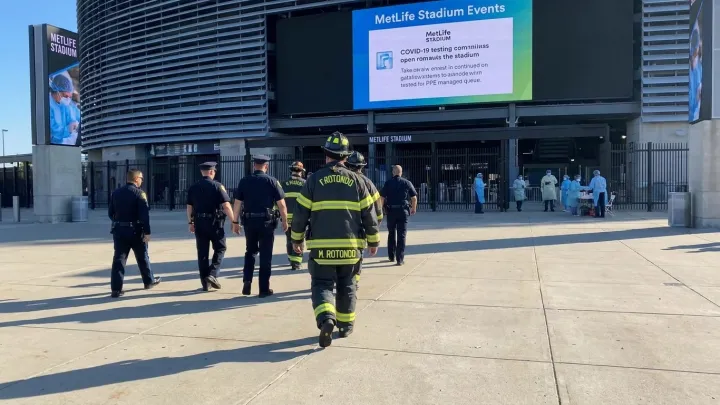
Nightmare is exactly what hospital planners expect. Stadium cheers, packed subway cars, and late‑night bar crowds form an almost perfect incubator for infection. With an estimated 1.2 million visitors headed for the metro region, facilities from Manhattan to Newark have treated the tournament less as a party than as a controlled biohazard experiment in a dense urban grid.
Quietly, the real action has been in the simulation labs. Emergency departments have spent years running full‑scale drills on measles clusters, meningococcal outbreaks, and vaccine‑preventable respiratory disease, guided by models of droplet transmission and basic reproductive number. Staff cycle through tabletop scenarios that fuse mass‑casualty triage with communicable‑disease containment, testing how fast they can isolate a coughing fan from a crowded waiting room.
The blunt truth is that crowd medicine now resembles counterterror work. Infection‑control teams review genomic surveillance protocols, negative‑pressure room capacity, and stockpiles of personal protective equipment, while regional command centers refine closed‑loop communication with transit police and stadium medics. Electronic health record alerts are being tuned to flag unusual clusters by nationality and recent travel, a sensitive task in a city already wary of stigma. For clinicians on the night shift, the real World Cup scoreboard will be hospital admissions, not goals.