An infection caught on duty now exposes a quiet flaw in global health confidence. A medical group says an American doctor has tested positive for Ebola after treating patients in the Democratic Republic of Congo, where sporadic flare‑ups of the virus continue despite years of investment in surveillance and response systems.
U.S. officials, led by the Centers for Disease Control and Prevention, describe the case as a contained occupational exposure, yet the incident underlines how fragile biosecurity remains when clinicians work at the edge of an outbreak zone. The physician, whose name has not been released, was reportedly following barrier nursing practices and wearing personal protective equipment, but still became infected after contact with confirmed Ebola cases in a treatment facility.
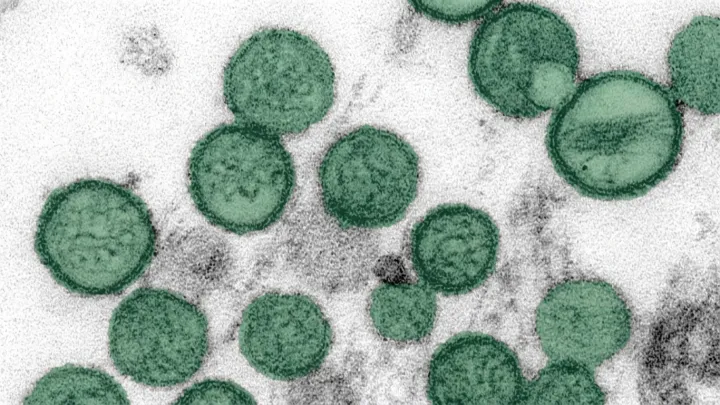
That breach, rare but not unheard of, exposes limits in infection control when viral load is high and procedures are intensive. The CDC is coordinating with Congolese health authorities on contact tracing and monitoring of anyone who may have been exposed, using standard case definition criteria and serial polymerase chain reaction testing to track possible spread. The doctor has been placed in isolation and is being evaluated for possible medical evacuation to a specialized biocontainment unit in the United States, according to the medical group.
For many experts, this single infection argues that frontline protection is still treated as a cost rather than as the hard core of epidemic strategy. Even with licensed Ebola vaccines and experimental monoclonal antibody therapies, outbreaks hinge on adherence to protocols, supply chains for protective gear, and the stamina of staff who work in heavy suits for long shifts. The case now forces health agencies to reexamine how much risk they are willing to ask individual clinicians to carry when they step into the hot zone.